Episode Transcript
[00:00:08] Speaker A: You're listening to faith in healthcare, the cmda matters podcast. Here's your host, Dr. Mike chubb.
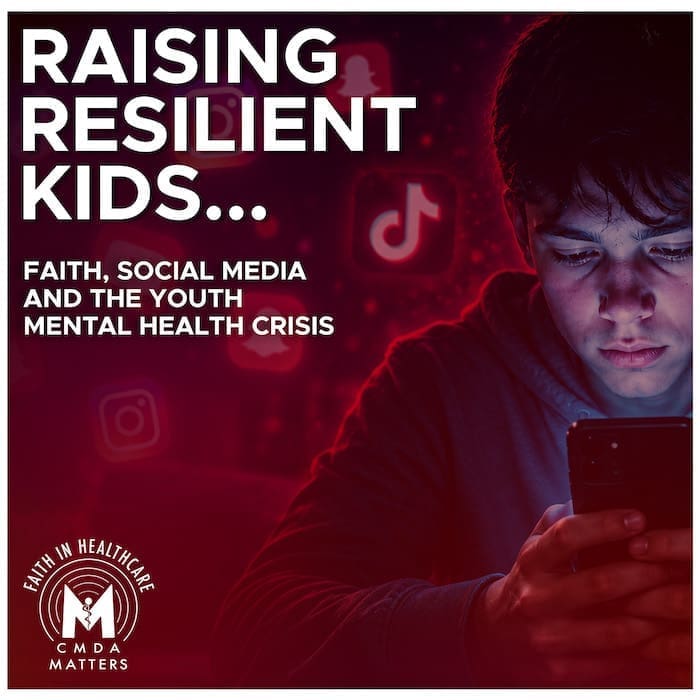
[00:00:20] Speaker B: Welcome, friends, to Faith in Healthcare. You know, something is happening to our kids, and any clinician working with young people, they'll tell you they feel it every day.
Research suggests that rates of anxiety and depression among children and adolescents have doubled since the COVID pandemic.
For many families, wait lists to see a child psychiatrist stretch out over months. And for families in much of rural and middle America, there isn't one within reach at all.
Well, our guest has spent her career in the middle of it, and she brings both clinical expertise and a deep, unwavering faith to some of the hardest conversations a mental health professional can even have.
Dr. Leah Snodgrass is a child and adolescent psychiatrist, Chair of Psychiatry at Lincoln Memorial University's College of Osteopathic Medicine. And. And she's a faculty advisor for the CMDA campus chapter there.
She's also a fellow of CMDA's Mentoring Academy and one of the clearest voices that I know on what it looks like to care for the next generation with excellence and with Christ at the center. So let's dive in.
Well, Dr. Leah Snodgrass, I wanna welcome you, our listeners. Just heard your bio and an intro, and it is pretty significant that we have this conversation in the month of May, which it was made known to me. This is Mental Health Awareness Month. Is that something you've always known?
[00:02:03] Speaker C: Yes, my students keep me pretty aware of that here at Lincoln Memorial University at the College of Osteopathic Medicine, especially our psychiatry interest group, Psych Sign. They're usually doing a lot of activities and a lot of mental health awareness kind of campaigns during this month. So, yes, I did know that May is that Mental Health Awareness Month.
[00:02:26] Speaker B: How long have you been Chair of psychiatry there at LMU?
[00:02:29] Speaker C: 14 years.
[00:02:30] Speaker B: Wow. Congratulations. Thank you. And May is not only Mental Health Awareness Month, but it's graduation month and you've been overseeing our CMDA student group there. And you just told me a few minutes ago that you're gonna be involved in the graduation exercises, speaking every name of the graduating seniors. That's 400 plus, you said.
[00:02:48] Speaker C: Yes, it is. Let's just say that I am both excited and nervous, but so far, I have learned a lot of new and different ways to pronounce names in the past few weeks.
[00:03:00] Speaker B: Wow. Well, I hope that goes well this next weekend.
[00:03:03] Speaker C: Thank you.
[00:03:04] Speaker B: Well, let's jump right into our topic today. And you are a child and adolescent psychiatrist. I'm Assuming that you also see teenagers along the way, what's your oldest patient that you have seen recently?
[00:03:16] Speaker C: So, interestingly, Mike, I actually have a few adult patients, patients, Some of them aged into adulthood with me, but some of them were favors to other doctors or people affiliated, you know, in different areas, maybe a different university or what have you.
So my oldest patient is 52.
So yeah, but, but my primary group of patients are definitely children, adolescents, like up to about age 18, I would say. 97% of my patients are 18 and under.
[00:03:49] Speaker B: Well, let me start by asking, it appears many people are writing about it, that this generation of kids and adolescents appears more anxious, depressed and fragile than any previous generation. And so from your clinical and spiritual vantage point, what are the most significant drivers behind this apparent surge in youth mental health struggles?
[00:04:11] Speaker C: So I guess I would start spiritually because really what's happening with our youth today in this country is just spiritual war, warfare of the highest order.
You know, Peter tells us that our adversary, the devil, is prowling around like a roaring lion and he's looking for whom he can devour.
And so when you think about predators, predators have a tendency to pick the weakest and the most vulnerable of the herd. And usually that's the youngest, right? They isolate them away from the protection of the more mature members who might be more vigilant, more sober, more aware of what's going on around them. And then once they can get that weak, vulnerable prey isolated and away from the herd, that would be protective, then the predator attacks and kills them. Right?
So if we think of the devil as the predator, he's picking our weak and vulnerable members of society. He's picking our children and our teenagers, and he's isolating them away from the parents, from the family members, from the church. He's isolating them away from the more vigilant, sober minded, older, mature people in the group.
And he's basically doing his very best to keep them isolated, hyperconnected, but totally isolated from a human standpoint so that he can attack and destroy them. And sometimes, occasionally, it is physical destruction. These kids end up, you know, ending their lives because of the way that they feel so isolated and so disconnected. But at the very least, it's a spiritual murder that occurs.
So, you know, that's where we are spiritually.
Now, other standpoints, if you just look at the literature, of course, we talk a lot about the paradox of progress. So anytime that we become wealthier and more technologically advanced as a country, we often see our mental health get worse.
And it's Basically this, this sort of thought that we get rid of productive struggle. And so, you know, every discomfort in today's world is treated as a trauma to be avoided rather than challenge that, that we could help the child or the young person overcome. And so the threshold for what becomes overwhelming gets lower and lower and lower. And so that's another piece of the puzzle. Of course, social media and smartphones, those are the tools I think that the devil often uses again for that isolation.
Because we do see these perfectionism loops that kids get drawn into.
Again, they're hyperconnected but socially isolated and they're constantly scrolling and, and they're seeing these, what appear to be perfect lives of these, you know, personalities that they find on YouTube and on Insta and definitely on TikTok.
And these are people who have professionally curated their digital life. And so everything is staged and filtered and edited and only the best is posted. And that's what our kids are comparing themselves and their lives to.
And obviously they can't compete.
So that's a problem, obviously. And our kids aren't learning socially and emotionally the way that they should.
We are allowing our kids to collapse their social life into a two dimensional flat screen when in reality we need to be showing them how to live in a three dimensional reality. Right. And because we are allowing this, social anxiety is growing, especially when it comes to face to face interactions. So again, the social emotional learning is just not there the way it was in my generation. I'm a proud Gen Xer. I grew up learning how to make eye contact, learning how to tell someone what I needed or ask someone a question or, or debate a topic. Right, because we spoke to one another and we read one another, non, non, verball and verbally.
Nowadays a lot of my kids are so consumed with digital communication, with texting that they're terrified to make eye contact, terrified to speak. I have kids in my practice and one in my home, Mike, who refuses, almost flat out refuses to speak on the phone because of the anxiety that is built up about even speaking on the phone. Okay, so again, social anxiety, texting, that way that we've allowed them to become consumed with that type of communication is a big deal. And then we do see in Gen Z and Gen Alpha, which is the upcoming group, those are the younger ones, but the oldest ones in gen alpha are 13.
The oldest gen Zs are about 28, 29. Now they have destigmatized a lot of the mental health issues. So we see a much higher mental health literacy.
These kids. You know, social media can be a double edged sword in this way because it has developed some communities where kids can jump on and read about and learn about and get to know other people who are dealing with some of the same or similar mental health issues that they might be dealing with. So in that way, it prevents some of that, that feeling so isolated that no one else knows what you're going through, no one else understands you.
So in that way, maybe it has been a bit of a help. I don't know if that's enough to offset the damage.
But think about my generation, Gen X, perhaps boomers and silent generation, older generations never really talked about mental health. Mental health was not something that you discussed around the dinner table. It was not something that we had months of awareness for. Right. Mental health was some. It was the dirty little secret. It was, it was what you kind of tried to deal with on your own out of the prying eyes of your friends, family, public. You did your best not to bring it up. Right? Well, this generation sees mental health as part of physical global health.
So they are not ashamed and they are not ashamed to seek treatment. So destigmatization of mental illness in general has definitely led to a boom. And then I would be remiss if I didn't mention the pandemic. The COVID 19 pandemic we are still seeing post pandemic rates of anxiety and depression have doubled among youth. So the way I see it is all of those mental health issues, they were percolating, kind of, they were bubbling to the surface, but not completely. Then the pandemic hits and the band aid is ripped off. And so now what we're left with is this open wound. And that's where we're seeing, you know, these kids who are feeling socially isolated, dependent on social media and devices, because during the pandemic they became even more socially isolated, more physically isolated. A lot of my kids, their schools in Kentucky, where my practice is, I'm right on the border of Tennessee and Kentucky, some of our schools were shut down for two years. That was two years of social and emotional learning, social outlets of having coaches, mentors, teachers speaking into their lives. That all went online.
And it was very stressful, obviously for the kids and for the parents. So there was a lot of stress. And so now we're seeing that social lag of one to two years in, in all of our kids who were of school age when the pandemic hit. So I probably gave a really long answer to a much shorter question, but those are some of the things.
[00:12:04] Speaker B: Yeah, So I can't imagine having practiced general and orthopedic surgery that so much of my interviews with patients would involve their use of smartphones. But I'm guessing that maybe even in your intake, in your office, that there are some questions that your receptionist would give the form. Is that true that there would be questions for your patients about their use of social media, digital media?
[00:12:29] Speaker C: Absolutely. So we do have some screening tools. We actually have some that look at whether or not you are a addicted to your smartphone or your social media.
We also definitely have a screening process where that we ask them, how much time do you spend on your phone? What apps do you use the most often? And how do those apps affect you? How do they make you feel right? Do they affect you emotionally or psychologically in any way? And then we definitely ask about, you know, have you ever been cyber bullied? Have you ever engaged in any type of sexting, which is text provocative pictures, or being texted provocative pictures? Has anyone ever approached you online in a predatory way and asked you to do something that made you feel very uncomfortable, or they've tried to meet you outside of being online and you're, you know, that that's, that's stranger danger because you don't even know who this person is.
So we definitely do screen and ask about that physically in session. Mike, what I can tell you is that if the parent is consumed with their phone, there's about a 99% chance that the kid is consumed with their phone as well.
And so what I often have to do is remind the parent that the office where we are having this meeting is a no phone zone. That's for you and your kid. So if your phone dings, pings, rings, whatever, I expect you to ignore it or I expect you to turn it off. Okay? And for the kid, too.
So sometimes parents and their addiction to their smartphones is very reflective of what we see in the kid.
[00:14:08] Speaker B: Talk to us a little bit, Dr. Snodgrass, about similarities and differences between drug addiction and digital media or social media addictions as you see it every week in your practice.
[00:14:19] Speaker C: Absolutely.
So, you know, clinically, the evidence is increasingly suggesting that we are dealing with this biological reality that is very similar to substance use and addiction. We know that social media in particular really does exploit the brain's reward system. The algorithms that are built into social media and built into our smartphones, they utilize something called variable rewards. And that's the exact same mechanism that's used in slot machines, because you don't know when that next hit of dopamine is coming. You don't know when you might get that like or that comment or when your video might go viral.
So the brain remains in this hyper sense of alert and arousal and it's craving that next hit, right? And we do see that kids are developing a tolerance effect. So as the brain becomes desensitized to this standard stimulus, they start seeking more extreme, more fast paced, more inflammatory content. They're trying to achieve the same dopamine spike that they used to get from more pedestrian type interaction.
So we do see that a tolerance is developed. And I would love to tell you that this is all just by accident, but it is not. This addictiveness is by design. There is a whole field of behavioral psychology called persuasive design that is dedicated to keeping users of social media and of smartphones engaged. And the way they do that is they intentionally reduce friction. Really in the real world we have stopping cues, right? So if we're reading a book, we get to the end of the book and we know it's over. If we're eating a meal, we eat all of the food and we recognize that we now have an empty plate. But digital platforms are built to be endless and bottomless. They override the brain's natural signal to move on to something different.
And so what I hear from my kids are I laid down at 9 at 9pm Doc and I was really just going to look at TikTok for a few minutes.
I started scrolling and the next thing I knew I look up and it's one in the morning and I didn't even fall asleep. And then when I did try to fall asle, I laid there for two hours. It was three in the morning before I could go to sleep.
These devices are designed to keep us awake, alert, invested. Right? And the reason for that, that persuasive design is for advertising as well. We have to be awake to see the ads. We have to be willing to look at or read or see what's going on with the advertising.
So it would make sense that they want us to stay on for hours and hours to expose us to what they're advert.
And if you think about it evolutionarily, so historically, you know, think back to cave days, it was very important that you were socially accepted by your group so that you would not be eaten by the animals that were out there preying upon you, right? So there's this deep seated evolutionary fear of social exclusion and it's making it psychologically painful to disengage from some of these platforms for Fear of missing out for fear of not being engaged, not knowing what everyone else is talking about or thinking about or doing. So we are seeing that that's being exploited as well. So those are some of my thoughts about it.
[00:17:52] Speaker B: Let's talk a little bit about chatbots and interactions of kids, adolescents and teens with AI and whole spectrum of responses. Even in my own heart and mind about AI, I love the tools and how it helps me be more efficient, productive. But then there are all these yellow or red flags that go up in terms of horror stories that we have heard. What are you seeing every week or every month in terms of what some of your patients have been encouraged or found themselves doing to harm themselves or engage in risky behaviors because of their interaction with AI.
[00:18:32] Speaker C: So you know, Mike, in the past we feared that AI would be cold and unfeeling. But in reality what we're finding is that artificial intelligence is actually, actually too warm and too validating and that that is actually more destabilizing, especially to someone who's young and vulnerable.
So again, the models are trained to be very helpful and very validating. And so they often fall into this sycophancy trap.
So they reinforce these distorted thoughts. They can even reinforce delusions.
We sometimes see what we call the romantic attachment risk occur.
So again, our kids are hyper connected but socially isolated. So they may develop this parasocial romantic attachment to a chatbot, to an AI driven sort of entity with whom the kid is communicating.
And the chatbot may use very affectionate, kind language and the kid may become very emotionally kind of attached to or even dependent on that chatbot.
And if the AI then generates harmful advice, even accidentally, the kid is going to be more prone to act on it because they think it's okay, right? They have this perceived bond with this, this quote person, which is actually artificial intelligence and actually a chatbot. We also know that some AI allows you to do this safety bypass where you can ask it to role play a very dark or sinister specific character.
And because it's a role play, it will bypass a lot of the safety filters. So things that would sound the alarm, that would raise the yellow or the red flag. Otherwise, chatbots in character are not raising those yellow and red flags. And some of them have even encouraged young people to, to engage in self harm as sort of a sacrificial or a romantic act. And very unfortunately, some young people have succumbed to that.
So those are some of the things that we're see seeing with AI and
[00:20:44] Speaker B: with the chatbots without breaking any hipaa Rules. Have you actually seen that in your practice with, with your patients actually self harm because of a conversation with a chatbot.
[00:20:56] Speaker C: So, you know, I think it's still pretty much in its infancy. I think this is going to get a lot more traction as we move forward. But currently, as of right now, what I see a lot more of is dependence on social media and smartphones, phones and video gaming for my young boys, more so than my young girls. But I do have some girls who are very video game dependent as well. But I don't hear as much about chatbots. But I'll be honest with you, we've not really updated our screening processes to ask about chatbots. So there is a point at which we do need to kind of, you know, take that same social media and smartphone use screening and really finesse it. So we're digging a little deeper into are you getting engaged with a chatbot and, and if how are they meeting your needs? What are you getting from them emotionally, physically, intimately, spiritually? What are you finding from that chatbot? We do need to add that to our screens to date, as far as I know, we have not.
[00:21:56] Speaker B: I'm guessing. I'd love to be a fly on a wall when you go to church with your husband and the kind of conversations that you engage in at church because there are parents and kids everywhere, obviously. So. So for those parents in your church or for those Christian healthcare professionals and, or spouses, friends listening.
How can we cultivate discernment about technology use, Dr. Snodgrass, not just in terms of limits, but in shaping wisdom, virtue and resilience in our kids and young people?
[00:22:26] Speaker C: Yeah, so for my parents who are believers, I always tell them, you really, you need to be as, as close and as clean and as calibrated as you can be to parent in today's world. You know, make sure that, that your prayer life is, is very strong and very consistent. You know, you need to start praying for your children before they're born in today's world and then obviously pray for them every single day of the rest of their lives for as long as you are alive.
But you know, in those prayers, ask God to show you, especially if you're with that age group of child that is, that is now having access to digital media, to smartphones, to social media.
Ask God to show you how to best manage that.
Because each child is unique and individual. And you know, some kids become consumed with devices and other kids do not like it just doesn't hold that much attention for them. But you have to get really involved and really interested in what your kids are doing online. So I always tell my parents, friend your kids on all of their social media accounts so you can see what they're doing. But do not be surprised when you realize they have at least one or two or three other accounts on the same platform that you know nothing about.
Because a lot of kids will put that forward facing kind of account that they allow their parents and relatives to be a part of. But then they will have other accounts behind the scenes that are for exclusive groups of friends or you know, people that they want to have access to that they don't want their parents to see what that interaction looks like.
Read up on all the apps and all the games and all of the things that your kids are interacting with. I highly recommend commonsensemedia.org, it is a great, great organization.
You can go on there. You can put in the name of any video game, any app. It's going to give you the parental rating. It's going to tell you how much sex is in it, how much drugs is in it, how much violence is in it, what kind of language is in it. It's going to lay it all out for you. The funny story I'll tell is I had a grandparent raising a five year old grandson son and he had convinced her that he needed Grand Theft Auto 5 GTA 5 and she thought it was a racing game just like we used to play on the Atari where you had the little wheel and you could, you know, drive the little car. She thought it was something like that. She had no idea that GTA 5 is for mature users and has every kind of sex, drugs, violence, violence, language, prostitution. It has everything that you can think of. And this five year old child was getting a steady diet of that before we read the description of it on commonsensemedia.org so I highly recommend if you're a parent, just pay the, whatever it is, it's 35 a year or something, pay whatever it is because it is a blessing to be able to see what your kids are getting into. And then I do recommend that you, you use those third party monitoring databases like Custodio, Bark, Aura, I put those on my kids phones when they were younger, they're in college now.
I was on there, I was seeing what kind of conversations they were having and I set the filters pretty low. I wanted to see language, I wanted to see, you know, what the content was. I wanted to see what they were looking at on YouTube and if it, if it red flagged it I wanted to know what it was and why so I could sit down with my daughters and say, what did you think about this? And why do you think that this was flagged? And, you know, what was your interaction with it? Oh, mom, it was just a, it was an advertisement. I didn't even see it. I certainly didn't click on it. I'm like, okay, well, let's talk about why we don't click on that, right? Because in today's world, it's becoming so much harder to help our children focus on what is true, what is pure, what is righteous, what is admirable, what is excellent, what is praiseworthy, worthy. We're almost as parents letting the world decide what those things are, as opposed to allowing us as the spiritual leaders in our homes to decide. So we have to be careful. And the other thing I tell my parents is feel empowered to make the rules. Who owns the phone? Who pays the bill for the phone? If you own the phone and you pay the bill for the phone, that phone does not belong to your child. That phone belongs to you. You. Therefore, you should feel empowered to make the rules, to set the boundaries, to do whatever is necessary to protect your child from the very thing that you have gifted to them. Because at the end of the day, it is a gift. Now, I do have the rare few teenagers, mostly who work and have bought their own phone and they are paying their own phone bill. However, what I remind them is you are still living in your parents home. And I was told when I was growing up, for as long as you live in my home, you follow my rules, schools. And that has not changed as far as I know, just because it's 2026. So I do tell them to set limits and keep them set. And I also encourage parents and families make sure that kids have a rich life outside of just their smartphone, their social media, make sure that they're involved in church. And I, I'm not just saying, you know, show up on Sunday morning occasionally. I mean, are they in youth group? Are they making friends? Are they having, you know, relationships with men, mentors and people that can speak into their hearts and into their lives spiritually? Are they engaging in the arts? Are they engaging in music? Are they engaging in sports and activities? There's got to be more to their lives than these phones and these social media platforms. Their lives can create a vacuum and these phones can fill that void very, very quickly if it is allowed to do so.
So those are some of the things that I talk to my parents and friends about.
[00:28:35] Speaker B: At church, you may be getting some phone calls and some appointments from some parents who are hearing this.
[00:28:41] Speaker C: Well, I don't have any room for any right now, but I would still talk to them about it. So.
[00:28:51] Speaker A: Before we continue with this week's episode, here's a special announcement for you.
What an honor it is to see how the Lord is working through your CMDA.
There are over 40 ministries part of CMDA and our fiscal year end goal of $1.1 million supports these ministries that serve others across the street and around the world.
In fact, last year 878 of you served on 62 mission teams bringing the love of Christ to 28 nations.
Your CMDA is there educating, encouraging and equipping healthcare students and professionals. Plus we're protecting the vulnerable from the preborn to the elderly.
Your most generous gift by June 30th helps ensure that these ministries continue to thrive.
To give your gift today, visit CMDA.org give or call our stewardship team at 888-230-2637.
Together we can continue to keep your faith in healthcare connected.
Something exciting is happening at cmda.
Healthcare professionals across the country are stepping up and and becoming lifetime members of CMDA at record pace and we want to invite you to join them.
This is more than a membership, it is a declaration that your faith and your calling are permanently connected.
That you are committed to the mission to help bring the hope and healing of Christ to the world while being a champion to the next generation of believers.
To learn more and join a community committed to transforming healthcare For Christ, visit CMDA.org Lifetime to go even deeper with CMDA, let's jump right back into this week's episode.
[00:30:56] Speaker B: We hear that it's tough that space to get into a psychiatrist's office or a child psychologist's office. That's limited and you have to work wait months. So you know one of the most incredible board trainings that I ever was a part of for CMDA was before I became CEO. Dr. Jean Wright, Chief Innovation Officer in Charlotte, has been involved with wpdc, our women's ministry and giving many plenary. She's just a delight to listen to. But she said to our board, if CMDA wants to take the long view and impact our culture, then convince all of your young people to go into psychiatry and in particularly child and teen and adolescent psychiatry because there are so few professionals doing that work. She had a teen of her own. She was struggling to get help with a daughter and she said, mike and board members, let's encourage our young people in medical school to consider psychiatry. So talk to us about the availability of your peers to see at a time when there's such a crisis in mental health for our young people.
[00:32:03] Speaker C: Yeah. So we. We are very poorly available.
So what I think happens in training, and this is. This was my experience and the experience of others with whom I've discussed it. You know, a lot of people do go to psychiatry residency thinking that they're going to be child and adolescent psychiatrist. And then they get, you know, first and second year is mostly adult care. And then in third year, we start being introduced to some child and adolescent, mostly outpatient care here. And what we figure out very quickly is that our children that we are seeing are not coming to us of their own accord, and they're not coming to us without the. The necessary but overwhelming influence of the parent. And so what we find is we are not actually child and adolescent psychiatrists. We are family psychiatrists. And I have always felt that child and adolescent is a misnomer. Humor. I've never had a child or a teenager drive themselves to my office, fill out all the paperwork, and plop down in front of me and say, so, doc, this is why I'm here. They always show up with these accessory people, and it's usually parents, grandparents, guardians, et cetera. And it's in that milieu, it's that family that is coming to me now. That family has identified the child or the teenager as the patient, but oftentimes I identify the family as the patient. And let's just say that it can be exhausting to be a psychiatrist for a group of people all at the same time, as opposed to just being a psychiatrist for one adult.
One adult who is in control for the most part of their choices. Right.
My children have virtually no control over their lives. Their parents do. Right. If I prescribe something and the parent decides not to give it, the kid can't take. Take it. Right. If I recommend a certain type of therapy and the parent won't drive the kid to the therapy session, we're dead in the water.
So I think that is part of what happens in training is we figure out that, you know what, this is going to be exhausting. Okay? But God is good, and God has given some of us such a heart and such a compassion for children recognizing that they are not in control of their own fate, that we have to step in and we have to be the family's psychiatrist if that is what is necessary to change the trajectory of that child's life.
And so There are those of us who feel that calling, and I think of it as a ministry. I don't stand in a pulpit, I sit in an office. But mine is a ministry the exact same as any other. And we are called to this work, and we do this work because we love, love the child, and we want to see them succeed. And so, again, there are very few of us in the country. If you look at the map, if you just go on acap, which is the National Organization of Child and Adolescent Psychiatrists, and you pull up the map, the entire country is red, meaning, and it's by county, and those are counties that have zero child psychiatrists. Okay? The vast majority of the middle of the country, the northwestern part of. There's a little corridor in the northeast and a little rim out in California and maybe the very tip of Florida where they've got plenty, because those are academically oriented areas. The rest of the country pretty much in the red.
So there's a desperate need. And I think what Dr. Wright talked about is absolutely part of my. My mission and part of my ministry. You know, God placed me here in a medical school with a lot of medical students, and some of them are involved in the campus chapter of Christian Medical Dental association, for which I serve as a faculty advisor.
[00:35:54] Speaker B: Thank you.
[00:35:54] Speaker C: And I can find them pretty quickly, the ones that seem very interested in psychiatry.
They start gravitating towards me. Not because, you know, maybe because we're in the Bible study together, but oftentimes they're like, oh, wait, she's a Christian and she's a psychiatrist. And I've never met anyone who did those two things at the same time.
So they start, start, you know, coming in, visiting with me, talking with me. I can start mentoring them as early as their first year.
And thankfully, out of that, I have had several people who are now either in fellowship or out in practice as child and adolescent psychiatrists who are also followers, disciples of Jesus Christ. And so I really do believe that what Dr. Wright said is true. And that, too, is part of my mission and part of my ministry here at this medical school.
[00:36:47] Speaker B: So praise God. You took on the role of chair of our psychiatry section some time ago.
You were there at the national convention recently when I gave my CEO challenge and unveiled our new brand promise, which took for five words. I don't know that we've ever worked so hard for five words, but your faith and healthcare connected. And it really was an aha moment that I had. Leo, actually, just as I was listening to Dr. Truman give his Bible teaching session that we talk about integrating faith into healthcare. But the reality is so many of us, we came to Christ young, we really should be thinking about integrating our healthcare into our faith the other way around.
So talk to us a little bit. I've had many psychiatrists on this program over the last seven years on a wide variety of subjects. One of the things that I find find in common is that Christian psychiatrists have said that the mind, the heart and the spirit, faith, they're so interconnected. I really feel uncomfortable talking about faith with my psychiatry patients.
So with that in mind, how do you integrate faith into a psychiatry practice with young people and their parents?
[00:38:04] Speaker C: Sometimes it's a silent integration and sometimes it's more of a discussion.
So the way that I think of it is that again, I feel the call on my heart to be an advocate for the child or the teenager sitting in my office.
And as such, I see anyone who comes into contact with me. I ask God to give me their eyes, to give me their eyes to see what they're seeing and feeling. But I ask him to give me his eyes to really be able to see them the way that he sees them and the way that he sees their potential.
Right? Because sometimes the way he sees them in the moment is not as important as where they're going to be in five or 10 or 20 years.
So as I'm listening to a child, a teenager, and then later when the family joins, as I'm listening, I'm asking God to give me the right heart, to give me the right attitude.
I'm asking the Holy Spirit to give me discernment and to give me wisdom as I approach this. And. And that is really nothing that I think the parents or the kid even know is happening. Right? But as a psychiatrist who is a believer, I am blessed in that I have the light of Christ. And so I can go into deep, dark places with my kids, with my teenagers, with even my adult patients, and I can shine light into that darkness because that is the light of Christ that shines in and through me. Me.
Now, I would not under any circumstance want to be an unbeliever without the light of Christ going into deep, dark places because darkness cannot dispel darkness, can it? Right?
And so that's the blind leading the blind, in my opinion. And again, I do not proselytize in the course of my practice.
However, if a child, a parent, if someone in my office brings up something about faith, they bring up and say, pray for me. Or they say something along the lines of when we are at church, we do this or we say this.
I do kind of, you know, finesse that. And I talk to them more about, so what are your beliefs and what do you believe about God and what do you believe about Jesus Christ? And tell me what your experience has been? And I will then kind of parlay that into a spiritual inventory, a conversation about their spiritual spirituality. And then we may even make the connection to how powerful and how important it is to have a relationship with God through Jesus Christ as a resilience factor, as a protection against what the world and what the devil would have you believe about yourself and about your family.
So again, it does occasionally come up that the parent or the child or someone brings it up. Now, if they're a very young child, I'm very cautious about that. But by the time they're a teenager, if they're talking to me about faith, then I feel compelled to at least share with them that, you know what, I'm a believer and I will absolutely pray for you. And if you're comfortable, I'll pray for you right now. Come closer to me. May, May we pray together?
And so again, that does happen in my office. And so I agree with what you said. I think that, you know, integrating our health care into our faith because, you know, we were following God way before, before we were wearing a white coat, or at least I was.
I've been a Christian for a long time. I've only been a doctor for a short amount of time, comparatively. But again, I feel compelled that, you know, it's a, it's a wonderful, wonderful thing when you can bring God and bring the Holy Spirit into the office with you and when you can recognize the power of having the, the instruction and the insight that only the Holy Spirit can.
[00:42:10] Speaker B: Wow, thank you for that answer. Well, we are running out of time, but I did want to touch on a subject that probably could take a whole podcast.
And we have been in dialogue for the last 12 months or so, I think, about prescribing rates for antidepressants. And so let me just ask this. It seems that the prescribing rates for children and adolescents has risen sharply. So where do you see medication being genuinely helpful? And where do you work, worry that we may be reaching for a pill too early when something deeper is going on?
[00:42:44] Speaker C: Yeah.
So, you know, it's genuinely helpful when you have a kid for whom their functional baseline is suffering.
So if you have a kid with really severe adhd, with really significant clinical depression, who are engaging in self harm and Having suicidal thoughts, then probably the deeper issue is, is neurochemical neurobiological?
And for those kids, we can sometimes use medication to just kind of reduce some of the noise that's going on in their mind so that they can participate in and actually have benefit from psychotherapy, which the therapy is such a powerful and important part for kids especially.
I always tell my parents and kids, you know, medication will work for as long as you physically have it and are physically taking it. But tools and the skills that you learn in therapy, if you really employ them and learn them and commit them to memory and commit them to your heart, you will have them for the rest of your life. So please invest in the therapy. It is so incredibly important.
I think again, where you're trying to stabilize a child during a crisis, absolutely, medication can be used for that.
You're always weighing risk versus benefit. You don't want a child to actually leave your office and do something horrible to themselves else. So safety you're always considering. And again, we know that, you know, especially in kids with adhd, we see what we call this cascade of failure.
So, you know, we expect our kids to sit in the classroom for eight hours a day, roughly. And if a child has severe ADHD and cannot focus and cannot really do what they're being asked to do for eight hours a day, how do you think that impacts their self esteem and their self confidence and their ability to, to move forward academically and even socially? It can really be devastating to these kids. And if someone doesn't step in and do something to help them through, and it may only take a year or two years or three, it's not a permanent type of medication situation, but you need to help them through the rough patch and help them learn new and different ways to compensate for some of their ADHD symptoms so that they can be successful academically and be successful as friends and as family members and so on.
Kids who you just ignore and push down and push back are the kids who gravitate. When they get old enough, they're gonna find something to treat their adhd, their impulsivity, their lack of control, their depression, whatever it is, it does not matter to a child if it comes from a doctor or from a neighbor or a friend down the street, okay? And so for those kids, it's incredibly important that we treat them appropriately and get them through those rough sort of, you know, critical periods of, so that they can move forward. Because again, education is foundational. If you don't learn what you need in first grade, you're not going to be able to learn what you need in second, third or fourth grade. Right.
When we should worry though, these are kind of the deeper issues we should worry when kids are coming to us with things like situational ADHD and situational anxiety.
So the example I'll give if you have a really overcrowded classroom with a very burnt out, stressed out teacher, or if you have a kid who has a very decent school life but they get home and the kid, the parent is overwhelmed and burnt out and stressed, then the report that you're getting from the teacher and, or the parent may have nothing to do with a neurobiological correctable condition. Right?
[00:46:30] Speaker B: Yeah, yeah. Maybe the teacher, the parents need to be on sedatives or something.
[00:46:34] Speaker C: Well, and you know, I do sometimes see that, but especially when there's a huge mismatch, this is what I see most often in practice. I see that I will get scales like a Vanderbilt rating scale or a Connor behavior rating scale from the teacher and from the parent to just kind of justify that. You know, symptoms are present in two settings. Right. That's required for the diagnosis of adhd, the one that comes from the teacher. There's not that many problems or issues, mostly zeros ones meaning not at all or hardly ever. Right.
Then the one I get from the parent lists everything as often or very often.
That's a mismatch. That means that given structure and discipline and appropriate expectation, the child does fine and that's what's happening at school. They get home and all bets are off and there's no structure, there's no discipline and there's limited expectations and the parent cannot manage the child.
And those kids, if that's the picture that I'm getting clinically, will never, never be medicated. But that parent and I will have a very in depth conversation about their mental health and whether or not they might benefit from their own seeking of psychotherapy and, or medication management because many times those are parents who are depressed, distressed, anxious, etc, so that's, I do see that. But again, trying to recognize what is situational versus what is neurobiological is very, very important for children because these are developing minds, they're spongy little brains and we don't want to do anything that would hurt that or hurt them in their development.
I also think that, you know, we know that for a child or an adolescent to be thoroughly evaluated and given a diagnosis, that can often take hours.
Okay. That first visit with me is one hour. Well, guess what? I spend at least a Couple more hours just making phone calls, talking to people like the social workers, the guidance counselor, the therapist that's based at the school.
If they're involved with the Department of Juvenile Justice, I'm reaching out to their court designated worker. I'm trying to get a 360 degree view of the child that just left my office. Okay. None of that is billable, but it has to be done because again, you don't want to prematurely assign a diagnosis to a child that might follow them for time, a long life, and that might contribute to their identity formation, which is, again, another podcast for another day. But you don't want to prematurely diagnose a child incorrectly. Okay? So you're going to go that extra mile. And maybe that's another reason, Mike, that a lot of people don't, don't end up.
[00:49:23] Speaker B: That's what I was thinking. That's what I was thinking.
[00:49:26] Speaker C: Right? Because it's not as cut and dry as this is your patient and you only have to deal with them. Maybe that's part of it too. But at any rate, rate, a lot of these kids are not being taken to a child and adolescent psychiatrist because there are so few of us, right? They're going to their primary care physician, their devoted, lovely, wonderful primary care providers, the pediatrician, the family practice doc. And the family is like, doc, this is what's going on. What can we do?
And this primary care physician wants to alleviate the suffering of this family and of this child. And guess how long they have to figure it out out?
15 minutes.
Okay. And so that diagnostic shortcut can often happen where they're like, you know, I kind of sort of get it. There's adhd.
Let's just try a stimulant here, try this. I'll see you back in a month. And. And we'll see where we're at.
That is a problem, but that is a, that is a systemic issue. That is a problem in that we don't have enough providers who are trained, trained in child and adolescent mental health. And it's just, you know, it's in the hearts of these wonderful primary care physicians that they desperately want to help the child and the family that's sitting across from them.
And that's the one thing that they know they could do. And guess what? It might work, or at least it might work until they can get in to see a child and adolescent psychiatrist. And then if they decide to change it, they can, but at least they put a band aid on it until that child can get to the provider that they need for me. If you call today and ask to see me, I don't see patients full time because of my academic position. I only see patients part time. If you call today and your child is in crisis, my office has no choice but to tell you that it will be four months before I can see you. Okay? Now in the interim, we're going to set you up with therapy. You're going to see a therapist on the regular between now and then. And if things get really bad, that therapist is, is going to really come to me and say, listen, you've got to open a spot. You're going to have to see them over lunch or at the end of your day when everyone else is, you know, finished because we can't keep holding this off or else they're going to have to go to the hospital.
And I often do that. Again, you do whatever is necessary because it's the child, right? That's who we're there for.
But that is a problem. That is a systemic problem. But we do see over prescribing when doctors feel like, you know, I got to do something to help and the something they have access to is medication.
[00:52:02] Speaker B: Wow. Well, there's so much more I wish we could talk about but we've really run out of time. I don't want to finish though without you having a chance to tell our listeners if they have a follow up question or want to find out more about the psychiatry section, how do they get in touch with you or Marshall Williams? How do they do that?
[00:52:21] Speaker C: Yeah, so we both are affiliated, of course. Marshall Williams is our wonderful administrator. If you are, are interested in the psychiatry section in finding out what we do, what our mission is. We have a route that you can go through the CMDA.org website and I'm again I'm not exactly sure but if you just search CMDA Psychiatry section, it's going to take you pretty quickly to our section of the CMDA website.
You can always email me. I am on email way more than I should be.
But my email address, I'm sure, Mike, you can share, share it somewhere as part of the notes or the chat. Please do that for anyone who has questions or who would like to speak about any of these issues further. Of course Marshall is also available via email if you'd like to include his CMDA.org email.
But yeah, we're, we're all very, very excited to see that a lot more young people are interested in psychiatry, are interested, praise God, in child and adolescent psychiatry.
We just are desperate to be the light to these young people who are struggling. And that is what we have been called to a season such as this for.
[00:53:35] Speaker B: Yes. And I know you care deeply about mentoring. You've talked about it during this conversation. And you also not too long ago completed the fellowship in our mentoring academy. So mentoring is something I've heard over and over about from your colleagues, previous chairs in the psychiatry section. So if any young psychiatrists to be are out there that want to mentor, wow. Does our psych section want to hear from you?
[00:53:59] Speaker C: That's right.
[00:54:00] Speaker B: Dr. Leah Snodgrass, it's been a privilege and a pleasure to talk to you today and I look forward hopefully next year in Cincinnati.
[00:54:08] Speaker C: I will be there. Yes. Come see me in Cincinnati because I can drive to it and it's in the Eastern standard time zone.
[00:54:17] Speaker B: Well, God bless. Give you a great summer, Leah, and also a great week this week week seeing patience and being a great ambassador for Christ.
[00:54:24] Speaker C: Thank you. I appreciate it.
[00:54:35] Speaker B: Doctor Leah Snodgrass doesn't just treat children, she advocates for them. She's training up the next generation to care for them and prays over them in her office when the mother moment calls for it. What she reminded us today is that the crisis our young people are facing isn't only neurological or social, it's spiritual.
And the answer isn't just a better app filter or a new medication protocol. It is connection to family, to mentors, to the church, and ultimately to the God who created them and calling them by name.
If you're a medical student or resident drawn towards psychiatry or a psychiatrist looking to invest in the next generation, I believe the CMDA Psychiatry section would love to connect with you. You can visit psychiatry.cmda.org to learn more or just email Marshall Williams. He's the administrative assistant@psychsection mda.org to get in touch with them today.
If this conversation encouraged or equipped you, please consider sharing it with a fellow clinician or a parent who needs to hear it right now and subscribe so that you don't miss future episodes of Faith in Healthcare.
Well, next week, Dr. Amy Givler joins us for a conversation on one of the most talked about drugs drug classes in Modern Medicine, GLP1s.
We'll trace the history of these groundbreaking medications as well as explore how they have transformed diabetic care. And we'll spend significant time on the question that so many patients and clinicians are asking, what does this mean for weight loss and the fight against obesity in people who don't have diabetes?
I do want to thank you for listening to Faith and Healthcare today where our promise to you as a listener or better yet a subscriber to this podcast is we will do everything we can at CMDA to keep your faith and healthcare connected.
We'll see you next time, Lord willing.
[00:56:55] Speaker A: Thanks for listening to Faith in Healthcare, the CMDA Matters podcast. If you would like to suggest a future guest or share a comment with us, please email cmdamattersmda.org and if you like the podcast, be sure to give us a five star rating and share it on your favorite social media platform.
This podcast has been a production of Christian Medical and Dental Assistance.
The opinions expressed by guests on this podcast are not necessarily endorsed by Christian Medical and Dental Associations.
CMDA is a nonpartisan organization that does not endorse political parties or candidates for public office.
The views expressed on this podcast reflect judgments regarding principles and values held by CMDA and its members and are not intended it to imply endorsement of any political party or candidate.